
Jul 2, 2019
I had a thought provoking, interesting and great time learning and networking on the ORLAU gait analysis course I attended last week.
I have done various gait analysis courses in the past, but this was a really helpful course in revisiting aspects of gait analysis. The course has a high ratio of Faculty experts to participants. This enabled us to work in smaller groups for the mind boggling interpretation of what felt like 100’s of graphs!!
But in reality, once I learnt to look for the simple answer and dust off the (what felt like decrepit) mathematic and physics areas of my brain – which have essentially lay untouched for many years – I surprised myself in being able to actually plot kinematic, kinetic and analyse EMG graphs. Even writing this I’m amazed at how much I learnt on this course.
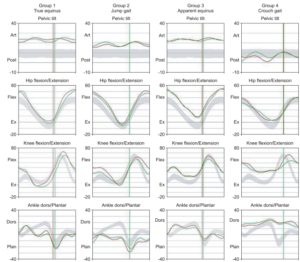
Sagital plane kinematic dataThe faculty included the great and essentially regal, Mr Andrew Roberts, an expert in ORLAU Gait Analysis, whose presentations were interesting and entertaining on both occasions I have heard him speak – I also now know he DEFINITELY doesn’t come from Dudley! I now better understand the principles behind hamstring length and crouch gait and have learnt a much better way of assessing this more accurately. Amongst other aspects of the clinical examination, as we had several opportunities to revisit examination in practical sessions.
The (not at all forgetful!) Mr Rob Freeman, shared a really interesting case study of a child pre and post SDR, and gave food for thought in terms of therapy input and how orthotic management along with SDR had a huge impact on the child’s gait pattern.
Sarah Jarvis (Physiotherapist) was an excellent Convener (if that’s the right term?!) of the course and entertained my need to discuss lots of the case studies in between the sessions and presented really interesting sessions on Orthotics alongside Tom Woods (Orthotist) and information about other gait analysis outcome measures, if you don’t work in a gait lab.

I revisited concepts that had been buried deeply on engineering concepts on forces, moments and powers, which alongside other topics helped me to understand gait from a different perspective. I better appreciated the forces our muscles have to generate when they have a short lever and how to interpret power and kinematic graphs to identify where there is tension in muscles and therefore aid in the decision making process for management.
Caroline Stewart and Neil Postans (Bioengineers), blew me away with their passion and expert knowledge of the intricacies of gait analysis and their expert delivery, making all aspects interesting and understandable to those of us with limited experience of the workings of a gait lab.
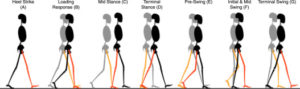
I revisited the gait cycle (many times with the help of Physiotherapist Darren Tinson), who was luckily very patient!! This helped me to look at the gait kinematics and kinetics in different planes and therefore gain a better understanding of all of the components at play and how to simplify and pick out the main limiting factors.
Simon Marchant (Clinical Scientist) managed to entertain the whole group with his theatrical presentation on recognising artefacts – his delivery helped me to remain focussed on a topic that was less relevant for me, but I still really enjoyed.
It was also interesting to go back through the gait cycle with Julie Reay (Physiotherapy Lecturer at Salford), her move from Children’s Community Physiotherapy to her current role is inspiring and it was great to be able to discuss cases with her. I look forward to visiting the Salford gait lab.
My take home lessons, as I mentioned earlier are related to clinical examination, understanding in more depth what effects and contributes to an atypical gait pattern. I am now more aware of the service at ORLAU, which will be of benefit to the children I see in my practice. The case studies and videos in different planes also reinforced my experience of changes in the trunk pre and post SDR and how improving the kinetics in gait enables better activation of lower limb muscles but can also improve the activation of the often underdeveloped abdominal musculature.
All in all, it was a great 3 days, which I would fully recommend. The venue was excellent, along with the provision of lunch and opportunities to network with orthotists, physio’s, consultants and engineers! That doesn’t happen very often in the field of Physiotherapy – but boy when you put those together in a faculty it produces a course of the highest quality.
I was even forgiven for my late application (sorry Sian Jones!). Thank you Sian and Sarah for organising a brilliant course and to the whole faculty for you time and expert knowledge.
I’m looking forward to visiting with my clients and to further my understanding of co-ordination of movement in Cerebral Palsy from the perspective of brain skills, with the observable gait analysis seen on 2 and 3D profiles.
I’ll be back……!
The ORLAU Gait Analysis is one of 26 clinical courses a year, and was organised by the Orthopaedic Institute, a charity at RJAH dedicated to providing funds for Research and Education Orthopaedic Institute. Contact me today to see how I can help your child.

Jun 6, 2019
I have worked as a Children’s Physiotherapist in many different settings, in specialist children’s hospitals, smaller general hospitals, in the community and now as an Independent Physiotherapist and have seen trends come and go, as they do in all areas of business, fashion and life.
Gwendoline Jul and Ann Moore wrote about this in the context of musculoskeletal physiotherapy in 2012 (1) and referred to the changes being related to socioeconomic factors, societal needs and desires (what do we want), as well as an increase in knowledge and evidence base. They summarise that a combination of hands on, and hands off therapy is best – sounds sensible!
So, what do we mean by “Hands-on vs Hands-off”
Well, in the context of Children’s Physiotherapy a simple explanation of hands-off, is where the predominant input is through review appointments and provision of a programme of exercises for parents to do with their child, or where a therapist provides activities where the child can practice a functional activity. Hands-on physiotherapy is a treatment session where the therapists handling helps guide the child’s movements in order to encourage and assist the child to move in new ways.

Hands-off therapy
Hands-off therapy, is typically review appointments with advice to parents on activities they can encourage their child to do.
There are many examples of where hands-off therapy is absolutely indicated. For me, this is when the condition is simple and it is easy for the child and parent to follow the instructed programme of exercises. For example, a child with a fracture or sprain – there is a localised injury in one area of the body. There may be weakness, but essentially the brain has already developed ways of moving which are not affected – the child has a typical brain. The child will have access to a wide variety of movements that have already been established. Intact sensory pathways are present, so they know where the limb is in space and they know where it is in relation to their body, their balance, visual and auditory feedback all provide information to support each other to build an overall understanding of their experience. They can maintain their sitting or standing position whilst isolating movement in their limb. They are also likely to be able to understand and follow instructions.
Typical development relates to a typical brain that enables us to move in a co-ordinated and effortless way. It supports learning new skills by way of repetition and practice.
Another example is a child who is delayed walking, and examination reveals good quality of movement, a good repertoire and variety of movements, demonstrating the building blocks for continued typical development – there are no concerns around this being a neurological difficulty. They may have been a child who was not so motor driven, or a child with less opportunities to develop those skills. Parents can be given advice on activities to encourage the child to move in different ways, to improve confidence and balance and off the child goes! You will see quick improvement when this is the case.
So, when does a child benefit from “hands-on” therapy?
To understand why children with a brain injury, for example a child with Cerebral Palsy, benefits from a “hands-on” therapy approach, it is helpful to understand a bit more about typical development.
So, children learn to move by exploration, they move and something happens, they repeat the movement, “….it feels different to move my leg that way”, “….o oh…I’m falling….…,I’m closer to that toy now – a ha!!”, “what happens if I try that again?”.
Typical development is the exploration of movement, movement for movement sake.

We know that typical development starts with a baby moving inside the mother’s womb. Studies looking at baby’s general movements born term and pre-term, describe that a typical baby is born with a variety of movement in their trunk, arms and legs (2). Variety is present from utero and continues as an infant develops.
Children who have developed typically have many combinations of movement.

Babies love to explore with sounds they make, their movement and their interaction. Typical development gives a child opportunities to move in many different ways, they develop lots of different combinations of movement, which is the basis to future progression. It is these combinations of movement that give you the quality and variability of movement seen in typical development.
All children with Cerebral Palsy lack the combinations of movement we see in typical development, different areas of brain lesion will affect how the brain learns to compensate for it’s specific area of difficulty.
This reduction in combination of movement further limits the child’s ability to explore and experience different movement opportunities. They may have attempted to move and instead of reaching the toy they fall over – they decide to not try again after several attempts. Instead they continue to repeat the same limited movement patterns and remain in their “safe” zone. Children learn very quickly to compensate for their area of difficulty (but their variety of movement / combinations of movement will remain limited), this may make them successful in moving but at the expense of developing more rich movement combinations.
Babies and children will move in the easiest way – even if this is detrimental to their future progress. They don’t know the impact on their future development!
So what can we do to help improve a child’s co-ordination.
Hands on therapy helps to guide a child to move in new ways, to help them to go where they wouldn’t go, because they know from experience that it doesn’t end up well. This helps a child to build up new ways of moving, which will help them to function better as they come up against gravity more.

Hands-on therapy
Quality of movement is important. If a child can increase the variety and the available combinations of their movements, they will be able to access a greater repertoire. The greater the variety of movement, the more a joint moves through it’s range and therefore limits the degree of contracture.
Repeating the same movement combination over and over, serves to further strengthen those muscles, making them in the long term become even more active and tighter. This limits future progression and can lead to a plateau in function being reached earlier.
A child is often missing movement combinations (as said earlier these movement patterns or the skills that are missing will be different for different brain lesions), but what we focus on is the most obvious symptom – muscle stiffness/spasticity. This is so obvious to our eyes, that we often miss the underlying movement difficulty that contributes to the stiffness and tension in the body.
Babies with Cerebral Palsy (in the main) aren’t born with stiffness, the stiffness evolves as a child comes up against gravity or tries to take part in tasks that the brain just can’t cope with – they have to use what they have – leading to more stiffness and limited movements . It is possible to see atypical co-ordination from before 20 weeks gestation, the stiffness in the muscles often isn’t the first sign (3).
We need to focus more on what a child is missing, rather than the most obvious symptom. Understanding the brain lesion and focussing on developing brain skills / co-ordination is the key.
So, hands on therapy in my opinion is vital for children with a brain injury, to help them to increase their movement repertoire. This isn’t to say that it should only be done by a therapist, parents can be taught to help their children move in new ways, alongside therapy intervention.
What the therapist brings is an in-depth understanding of the child’s movement difficulty, to understand why a child seems to go stiff when they stand, but not when they are crawling, to understand what areas of co-ordination are missing or what difficulties the child may have when they need to do 2 things at once (for example to sit up and talk at the same time, they may be able to sit independently, but they need help to sit when they are talking).
Hands on therapy enables a therapist to feel what is happening, to guide and support a child’s movement, to understand where the child’s difficult zone is and how this links to their specific brain lesion and then to engage and encourage a child to go into their difficult zone in order to learn new skills.

Hands on therapy can also be helpful for both of the above examples of a child with a typical brain, if the injury is old and the child has learnt new ways of moving. The therapist can help to guide and develop movement patterns. I certainly benefit from hands on guidance to encourage me to use different combinations of movement when I am in an exercise class – in fact I would benefit from some intensive sessions to help me re-balance my muscle activity around my trunk and pelvis (I’m sure I’m not alone!!). Imagine if I also had a brain injury complicating that muscle imbalance – I would need much more hands on help.
The decision about hands-on or hands-off shouldn’t come from a therapists preference, it should come from an understanding of the child’s difficulty, the capability of the brain to learn new skills and working in partnership with families to identify the best way to harness a child’s potential.
Hands-on therapy to continually find ways to develop skills is really important, but so is the knowledge this then imparts to families, to be able to continue those principles as much as they are able to in every day life and to make the best decisions regarding a child’s functional activities that will both promote participation and long term function.
So, in essence there is a time for both – both are equally important. But it is important to remember that hands on therapy encourages the child to move in new ways, to improve the variety and combinations of movements possible to help children achieve their potential – without it a child will use what they have.
I completed a MAES Therapy course 3 years ago and this has really helped my understanding of brain injury and how typical development evolves for a typical brain and that following a brain lesion you can no longer work through typical stages of development (tummy time, 4 point kneeling, 1/2 kneeling), you need to understand the individual child’s difficulties and which skills they are missing, which will relate to their brain lesion. The management will of course be different for different lesions, as different parts of the brain are responsible for different skills.
If you are a therapist reading this, I highly recommend completing a MAES Therapy course. , it has truly changed every aspect of my assessment, understanding and therefore management of children with a variety of disorders, not limited to neurodevelopmental disorders. You can follow this link if you are a parent interested in learning more about MAES Therapy
Other approaches that offer hand-on therapy/intensive therapy are; Bobath Therapy and Constraint Induced Therapy amongst others. Each approach has a different basis for it’s intervention – it is not the intention of this blog to compare approaches – but instead to highlight the importance of therapy intervention
The information contained in this blog is my personal opinion and is written with the aim of sharing how important the physiotherapy service is in developing the skills of children with neurodevelopmental conditions like Cerebral Palsy and represents my personal and professional opinion at the time of writing.
Helen King Children’s Physiotherapy offers in-depth movement analysis and hands-on therapy for those children who would benefit from this, click here if you would like to learn more about my services.

References
1) Hands on, hands off? The swings in musculoskeletal physiotherapy practice Musculoskeletal Science and Practice June 2012Volume 17, Issue 3, Pages 199–200 https://www.mskscienceandpractice.com/article/S1356-689X(12)00059-8/fulltext
2) The qualitative assessment of general movements in preterm, term and young infants – review of the methodology. https://www.sciencedirect.com/science/article/abs/pii/S0378378297000923
3) Predictive Value of General Movement Assessment for Cerebral Palsy in Routine Clinical Practice. Gunn Kristin Øberg Bjarne Koster Jacobsen Lone Jørgensen. Physical Therapy, Volume 95, Issue 11, 1 November 2015, Pages 1489–149 https://academic.oup.com/ptj/article/95/11/1489/2888271